Wisconsin Reconstructive Prosthodontics
Complicating Factors in Adult Gum Disease
As discussed elsewhere on our website, gum disease can become quite destructive for patients if untreated for an extended length of time.
Unfortunately, for some patients, certain pre-existing conditions can actually accelerate certain aspects of the overall disease process. For the patient pictured here in our treatment series, the extreme amount of flaring is caused by an orthodontic issue (Class II Malocclusion) that wasn’t treated during the patient’s childhood or teenage years.
Back then, it is likely that long term harmful effects of poor orthodontic alignment and occlusion were not yet evident. It is not uncommon for patients to delay traditional orthodontic treatment until adulthood… usually for economic or convenience reasons (youngsters and teenagers don’t like braces).

Multiplicity Factor
As this patient’s need for gum disease treatment increased, the severity and overall functional impact of the disease process was accelerated by an uncorrected faulty bite.
Malocclusion can cause unwanted lateral (sideways) forces on our tooth structures. For patients who have severe alignment problems but no gum disease… tooth breakage can be a common event.

As this patient’s Gingivitis slowly developed into Periodontitis (advanced gum disease), the accumulation of calculus, plaque and tartar caused bacteria seepage into the periodontal pockets, destruction of periodontal ligament attachment and loss of bone surrounding each affected tooth structure. Because of lateral forces, however seemingly insignificant (during younger years), routine biting and chewing slowly and predictably “pushed” the upper anterior teeth to flare.
In the profile photo it can be readily seen how routine biting, chewing and eating can become difficult. Cone beam Ct Scans were used to provide Dr. Winter and the patient the best diagnostic and planning capabilities possible.
A relatively young patient, he sought treatments that would best eradicate the disease process and fortify tissues lost during extractions (bone and gum tissues).

Tissue Removal – Replacement Surgeries
The adjacent photo shows the progression of mid treatment goals. All upper teeth have been extracted with bone graft products being used as needed to create a healthy, plump ridge of bone.
A variety of provisional and traditional implants can be seen here that enable the patient to have temporary teeth while final healing and osseointegration is completed.

The specific configuration of implants and implant sizing is based upon the technical data derived from the virtual treatment planning made possible with the 3D Ct Scans. This type of planning eliminates the guesswork of determining where implants belong and don’t belong.
Guided Tissue Regeneration membranes are used routinely with bone regeneration products to control the development of desirable tissue, both hard and soft (bone and gingiva).
Individual implants are placed into the “new tissue” when healing has been confirmed. At the time of each placement additional graft material is used when indicated and the gum tissue is re-sutured to develop a uniform level of gum tissue.

Healthy Bony Ridge
Final abutments have been fitted onto the implants. The two mini implants that were used to secure the temporary denture used by the patient during the healing process remain. Tissue grafting and implant site development occurs differently for patients who are undergoing a full arch reconstruction.
In some cases all of the extractions, grafting and implant placements can occur during a single appointment.
In other cases, sites may be developed in an incremental fashion, as needed, to assure a patient is never toothless. Provisional or mini implants are often used to secure temporary acrylic teeth that are eventually replaced with a final, porcelain bridge.

Mandibular Reconstruction
Once the upper arch implant procedures were completed and fitted with abutments and a temporary bridge, edentulation and initial implant site preparations were begun for the lower jaw.
The adjacent picture shows the removal of all diseased tissue. Grafting products, GTR membranes and implants were placed and sutured in. The unique placements for the lower implants correspond to the implant configuration that was developed with the 3D virtual planning software.
As with the upper jaw, the software was used by Dr. Winter to “virtually” locate the most robust areas on the mandible. Uniquely sized implants were selected for each implant location and placed “virtually” with utmost precision that could be viewed visually…. before surgery was begun.

Combining Procedures
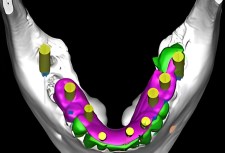
The adjacent photo shows a 3D scan of the patient’s fully edentulated (total tooth removal) lower jaw. The yellowish elements represent dental implants. The selection of each implant is based upon the tissue characteristics of each implant site, thereby ensuring maximum functionality…. no “one size fits all” type of dentistry.

Notice how the posterior areas (rearmost) of the lower jaw have substantially wider implants than those located in the anterior (front area). These sizing relationships mimic what Mother Nature normally provides. Mismatching an implant for a particular tooth location can lead to problems. The assumption that all implants can be the same size can also affect treatment outcome. Our next picture provides a reflected view of the patient’s new mandibular porcelain bridge. The underside of the bridge reveals how the abutment interfaces are designed to match or fit each individual abutment.
Based on the patient’s experiences with the temporary try-in acrylic bridge, he elected to have certain areas of the porcelain tinted with natural gum colors that provides an appealing cosmetic result.
The second mirrored view shows the alignment of a 3 section segmented upper bridge. Upper bridgework is commonly fabricated in segments that provide a better distribution of biting forces across the entire jawbone or bony ridge. Because the biting forces between different areas of the upper jaw vary significantly, improperly designed segments can lead to bridge failure.
Dr. Winter’s prosthodontic analysis of the patient’s characteristic biting forces determine the number of and size (span) of each bridge segment. During the try-in phase with acrylic temporaries, the distribution of biting and chewing forces is reassessed to confirm an efficient bridge design.


Final Fitting and Adjustments
The permanent restorations (final bridge products) are placed with temporary cements to assure additional opportunities for final adjustments necessary for obtaining the best possible bite and occlusion throughout all areas of the jaws.
The segmenting of the upper bridge, as mentioned above, facilitates the final adjustment phase. The original design of the patient’s upper bridge was modified to accommodate “lip and smile behaviors” that were changed somewhat with a bridge that followed the concept of Rules of Golden Proportion.

Call 414-464-9021 for information on any of our services.
Check out our Dental Blog >>
Read our Patient Case Studies >>
Hampton Dental Associates is proud to offer affordable dentistry programs to help you regain your perfect smile.
Learn more about our affordable dentistry options.